|
Focus on: 11q-
11q-, 13q-, trisomy 12 and 17p- are the most common CLL abnormalities detected by the diagnostic tool florescence in situ hybridization (FISH). Approximately ten to fifteen percent of CLL patients have 11q- either as the sole chromosomal abnormality or as the predominant abnormality. 11q- is associated with a short time to treatment from diagnosis and short periods of remission.
There are at least two contributing factors to the peskiness of 11q-. Patients with an 11q- abnormality often have large lymph nodes, also known as bulky disease. This means that the CLL cells reside primarily in the lymph nodes and are protected by their microenvironment (the environment in which the cells dwell and interact with other cells and molecules). It is much more difficult for drugs to eliminate these cells when they are under microenvironmental protection.
 | |
(http://ghr.nlm.nih.gov/gene/ATM)
Image of chromosome 11. The portion highlighted by the yellow arrow is where the ATM gene is located and where abnormalities and deletions occur in CLL.
|
Secondly, the ATM gene (ataxia telangiectasia mutated), located in the region affected by 11q- abnormality, is generally deleted or dysfunctional. A properly functioning ATM gene helps to control the rate at which cells grow and divide and is responsible for repairing defects or breaks in DNA. Much more needs to be learned about ATM and other genes in the 11q- region to fully understand its role in 11q- CLL. While genetic research continues, scientists are taking other measures to overcome the 11q- obstacle.
What we know about 11q-:
- 11q- is highly sensitive to FCR-like therapies even in older patients.
- Less intensive therapies prior to FCR-like therapy do not influence response.
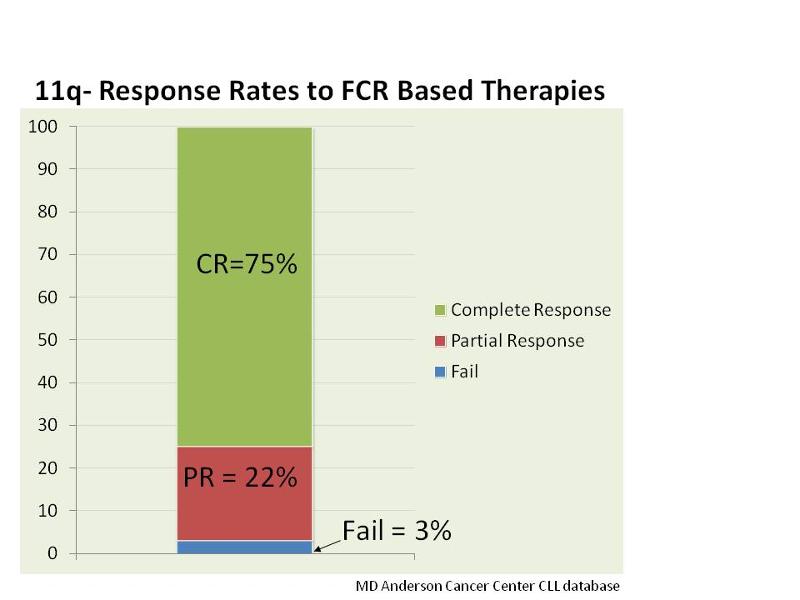
- 11q- patients have a high complete remission (CR) rate but shorter remissions than average (see figures below).
- Patients who are minimal residual disease (MRD) positive after treatment have shorter remissions than those who are MRD negative.
- Relapse is currently inevitable.
- The survival rates are the same as other genetic markers except for 17p-, even though 11q- patients have shorter remissions.
Short remissions and inevitable relapse may be partly attributed to bulky disease. Consolidation therapy, which is treatment given after initial therapy to maintain control of disease and enhance the remission, may help change the current statistics. New drugs like lenalidomide and BCR inhibitors are being looked at as potential consolidation therapies. (For more information on BCR inhibitors, click here.)
Also, BCR inhibitors force CLL cells from lymph nodes and into the blood stream where they are more susceptible to treatment. The hypothesis is that BCR inhibitors can reduce bulky disease, thereby eliminating MRD and prolonging remissions. A consistent, sustained decrease in lymph node size has been seen, but should not be considered indicative of full clinical trial results. More data and time will provide answers.
While progress has defintely been made in the understanding of 11q-, there is still more work to be done.
Going forward:
- A better understanding of the ATM gene and 11q are needed with further investigation of DNA repair capabilities of ATM. The goal is to eventually exploit this defect.
- BCR inhibitors will continue to be analyzed.
- Other new agents need to be explored in 11q- patients.
| 






