October 2014:
HPV and ENT
November 2014:
Non-stone Salivary Disorders
December 2014:
Non-stone Salivary Disorders
|
Our E-Update Newsletters are designed to provide brief, practical, clinical updates in areas where we all struggle in managing our patients. To view past issues, please visit our Archives. |
November 2014
F. Johnson Putney Lectureship in Head & Neck Cancer
January 2015
Charleston Sleep Surgery Symposium
March 2015
Pediatric ENT Update
Temporal Bone Dissection Course
May 2015 Southern States Rhinology
Charleston Magnolia Conference
July 2015 The Charleston Course: Otolaryngology
Literature Update
For program brochure, registration form, and more, please visit our website.
|
We want to hear from you!
We welcome your feedback on our newsletter articles as well as any ENT questions you may have. If there are topics you are interested in learning more about, please
|
|
|
The terms oral and oropharyngeal have been used synonymously over the years regarding risk factors and outcomes. Recent evidence shows these two locations for head and neck squamous cell carcinoma to be quite different and divergent in risk factors, incidence, diagnosis, treatment and outcomes. In this month's E-Update, Terry A. Day, M.D. reviews the latest evidence to clarify these terms.
Dr. Day's Head and Neck Oncology division will host the 29th Annual F. Johnson Putney Lectureship in Head & Neck Cancer on November 7, 2014. This half-day of lectures and discussion is for the practicing otolaryngologists. Conference and registration info is forthcoming and will be on our CME website page.
More about Dr. Day follows the article below and is on our website. Your feedback or questions about the E-Update articles, your patients, or any other ENT issue are always welcome. Write to us at entupdate@musc.edu. Please forward this E-Update to your colleagues who may be interested.
Many thanks for your continued interest and support.
Paul R. Lambert, MD
Professor and Chair
|
|
 |
Terry A. Day, M.D., Vice Chair and Director, Division of Head
and Neck Oncologic Surgery, MUSC
|
Oral vs. Oropharyngeal Cancer, Compare & Contrast
| |
Historically, many researchers and clinicians have grouped oral cavity and oropharyngeal cancers all together calling them "oral cancers". It is now quite clear that oral cavity cancer (OCSCC) and oropharyngeal cancer (OPSCC) are two distinct cancers that differ in anatomic location, patient demographics, etiopathogenesis, presenting symptoms, treatment and survival.
Anatomy
Anatomically, the oral cavity consists of the lips, buccal mucosa, floor of mouth, alveolar ridge and gums, anterior 2/3 of the tongue, hard palate, and the retromolar trigone. Separate and distinctive, the oropharynx consists of the soft palate, base(or posterior 1/3) of tongue, tonsils, palatoglossus folds, valleculae, and the posterior pharyngeal wall. The anatomic border separating the two is, from above, the junction of the hard and soft palate, and from below, the circumvallate papilla. (FIGURE 1)
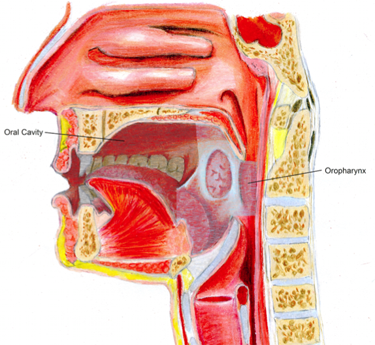 | |
FIGURE 1: Oral Cavity and Oropharynx anatomical locations.
|
Epidemiology
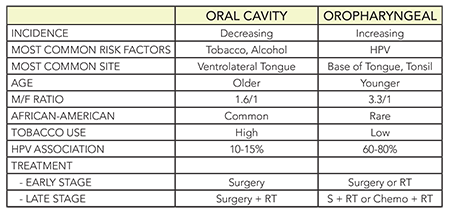
The incidence of oral cancer is decreasing while the incidence of oropharyngeal cancers is increasing. Patients with oral cancers (OCSCC) are more likely than oropharyngeal cancer (OPSCC) patients to use tobacco and alcohol, have less formal education, be African American, and to be in a lower socioeconomic level. (TABLE 1) Conversely, OPSCC cancer patients are more likely to have an HPV-associated cancer, are younger, more likely to be male, have a history of more oral sex/partners, be a non-smoker, European American, and at a higher socioeconomic status. (TABLE 2) Only about 15% of OCSCC are HPV positive while about 65% of OPSCC are HPV positive. Survival also appears to be lower in OCSCC than in OPSCC.
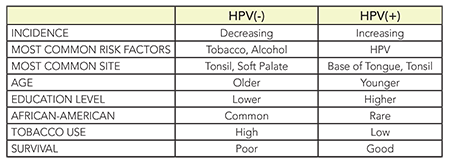
Interestingly, the OPSCC demographics are separated by HPV status. Thus, HPV negative OPSCC patients are more likely to be smokers, African American, older and lower numbers of oral sex/partners than the HPV(+) OPSCC patients. (TABLE 2)
TABLE 1: Oral Cavity vs. Oropharyngeal Cancer
TABLE 2: Oropharyngeal Cancers HPV(+) vs. HPV(-)
Diagnosis
Oral Cavity Cancer
Patients with OCSCC have historically been known to present with mouth soreness or red and white spots in their mouth. An example of an early T1 oral cavity cancer arising on the ventrolateral oral tongue is shown in FIGURE 2.
Oropharyngeal Cancer
Recent evidence suggests that patients with OPSCC typically present with a sore throat or neck mass. In a recent study, the majority of HPV(+) patients presented with symptoms related to the neck mass, such as a swelling they noticed while shaving, rather than a symptom related to the primary site. FIGURE 3 shows a typical appearance of an obvious OPSCC that was found to be HPV positive. In contrast, the HPV(-) patients appeared to have earlier onset of primary site symptoms such as dysphagia, globus sensation, odynophagia, otalgia and sore throat with neck mass being a less common presenting symptoms. (TABLE 3) Occasionally, the HPV(+) patients present with a neck mass and it may be cystic in appearance confusing the radiologist and clinician into thinking this is a branchial cleft cyst although eventually it is found to harbor squamous cell carcinoma(SCCa). In the setting of an unknown primary but fine needle aspiration of the neck reveals SCCa, imaging is employed and if no primary site is delineated, the authors advocate transoral robotic base of tongue excisional biopsy with tonsillectomy for definitive diagnosis.
 | |
FIGURE 2: Squamous cell carcinoma presenting as an area of erythroplakia on the ventrolateral tongue in the oral cavity.
|
 | |
FIGURE 3: Classic appearance of HPV associated OPSCC
in a non-smoker.
|
TABLE 3: Initial presenting symptoms of patients with OPSCC
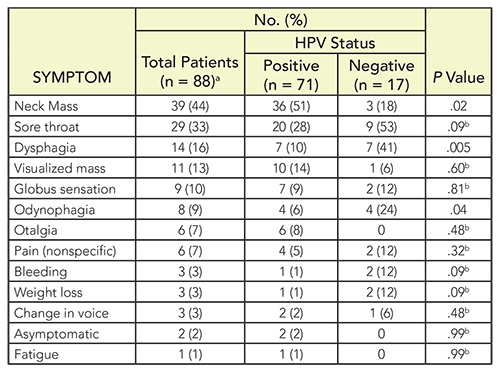 | | From: McIlwain, et al: JAMA Otolaryngol Head Neck Surg. 2014;140(5):441-447. doi:10.1001/jamaoto.2014.141 Published online March 20, 2014. |
Imaging
The large majority of OPSCC occur on the tonsil or base of tongue. If a lesion is not visible on physical exam a CT or MRI can be performed to the primary site. A CT/PET scan is performed often by the authors in late stage disease to evaluate for distant metastasis and/or to further delineate the primary site and/or nodal metastasis. FIGURE 4 shows the common finding of a cystic PET negative neck mass and small primary site in oropharynx of HPV positive OPSCC.
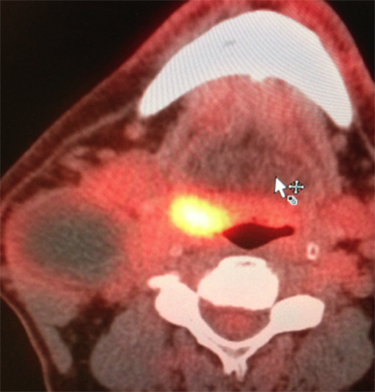 | |
FIGURE 4: Cystic neck mass with low FDG uptake with primary HPV associated OPSCC in base of tongue/tonsil.
|
Viral Testing
HPV testing is now the standard of care for all patients with OPSCC and/or an unknown primary. There are many types of HPV and the most common high-risk types related to cancer are HPV-16 and HPV-18. While work continues to identify a standardized, reliable and inexpensive detection assay, current testing may include p16 immunohistochemistry, in situ hybridization, PCR, E6 Serum Antibodies; and combinations thereof. The p16 detection is highly sensitive and is the most common method used at the authors' institution while in-situ hybridization is more specific.
Treatment
The standard of care for treatment should follow the NCCN Guidelines when possible and appropriate for the individual patient. Multidisciplinary care is important and should include surgery, radiation, medical oncology, dental oncology, and speech pathology among others. Treatment remains stage directed and, as yet, no modifications are recommended based upon HPV status thus all cancers(HPV(+) and HPV(-)_are treated according to NCCN guidelines.
The majority of both early and late OCSCC are treated surgically with clear 1-2 cm margins and neck dissection when clinically evident nodes or increased risk of occult metastasis. Advanced stage OCSCC(Stage 3/4) requires multimodality treatment with surgery as the initial treatment and finds surgical pathology dictating the need for adjuvant radiation or chemoradiation. The treatment decision-making in OPSCC is slightly more complex. For early stage cancers, either radiation alone or surgery alone is indicated while advanced staged cancers require combinations of either surgery followed by radiation or concomitant chemotherapy and radiation therapy. (TABLE 2) Decision-making in this scenario is difficult as one cannot predict the functional and curative outcome prior to treatment. When surgical resection is undertaken, several types of surgeries can be performed including the two common transoral methods: transoral robotic surgery (TORS) and transoral laser microsurgery (TLM) as well as the traditional approach (TOHS), transoral human surgery as coined by Dr. Joshua Hornig.
The authors often consider surgery when there is significant potential for downstaging and avoiding either radiation or chemotherapy and also when there is low risk to the soft palate (reducing velopharyngeal insufficiency) and low risk of injury to the neurovascular bundle of the tongue (reducing speech and swallowing deficits). A neck dissection is typically performed when there is clinical nodal disease or the risk of occult metastasis is significant. The findings of the neck dissection can lead to upstaging/downstaging and help determine the need for adjuvant treatment. Whenever radiation therapy is done on the oral cavity or oropharynx, it is recommended to be either IMRT or 3-D conformal RT.
Summary
Cancers of the oral cavity and oropharynx represent more than just distinct anatomic sites. The etiopathogenesis, diagnosis, treatment and outcomes have been diverging for over a decade. It is important for the diagnosing and treating physicians to be aware of these differences and provide the multidisciplinary care and education necessary to optimize outcomes. Treatment depends on the location and stage of the cancer. Vaccination to prevent HPV infection may have the greatest potential to reduce the morbidity and mortality of oropharyngeal cancer that so far is rising in the United States.
Benjamin Murphy, B.S. and Terry A. Day, M.D.
Medical University of South Carolina
Visit the MUSC Head & Neck Oncology website
|
- REFERENCES -
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 2010;363:24-35.
- Chaturvedi AK, Anderson WF, Lortet-Tieulent J, et al. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. J Clin Oncol 2013;31:4550-9.
- Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol 2008;26:612-9.
- Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol 2011;29:4294-301.
- D'Souza G, Kreimer AR, Viscidi R, et al: Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 356: 1944-1956, 2007.
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 2008;100:261-9.
- Gillison, M.L., et al., Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst, 2008. 100 (6): p. 407-20.
- Gillison ML, D'Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst 2008;100:407-20.
- Gillison ML. Human papillomavirus-associated head and neck cancer is a distinct epidemiologic, clinical, and molecular entity. Semin Oncol 2004;31:744-54.
- Haughey, B.H., et al., Transoral laser microsurgery as primary treatment for advanced-stage oropharyngeal cancer: a United States multicenter study. Head Neck, 2011. 33 (12): p. 1683-94.
- Kreimer AR. Prospects for prevention of HPV-driven oropharynx cancer. Oral Oncol 2013.
- McIlwain, W.R., et al., Initial symptoms in patients with HPV-positive and HPV-negative oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg, 2014. 140 (5): p. 441-7.
- O'Sullivan B, Huang SH, Perez-Ordonez B, et al. Outcomes of HPV-related oropharyngeal cancer patients treated by radiotherapy alone using altered fractionation. Radiother Oncol 2012;103:49-56.
- Smith, D.F., et al., Human papillomavirus status of head and neck cancer as determined in cytologic specimens using the hybrid-capture 2 assay. Oral Oncol, 2014. 50 (6): p. 600-4.
- Vermorken JB, Psyrri A, Mesia R, et al. Impact of tumor HPV status on outcome in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck receiving chemotherapy with or without cetuximab: retrospective analysis of the phase III EXTREME trial. Ann Oncol 2014.
|
About Dr. Day...

Terry A. Day , M.D.
Professor; Vice Chair, Clinical Affairs; Director, Division of Head and Neck Oncologic Surgery; Wendy and Keith Wellin Endowed Chair in Head & Neck Surgery; Director, Head and Neck Tumor Center
Advanced M.D.: University of Oklahoma
Health Sciences Center
Residency: Louisiana State University
Medical Center
Fellowship: University of Bern in Switzerland
Special interest: Skin cancer and tumors of the head and neck region
|
|
|
|
|