Thyroid nodules affect nearly 13 million Americans and are six times more common in women than men. They can be difficult to diagnose because they often do not present signs or symptoms. Most nodules are small and are often found incidentally during a routine physical or imaging for an unrelated condition. Though most thyroid nodules are benign, a large percentage of these patients will require surgery for either diagnostic or therapeutic purposes.
Until recently, surgery for thyroid nodules had not changed much since Theodore Kocher developed the classic techniques of thyroid surgery 90 years ago. However, in the last few decades there has been a period of innovation with the advent of "minimally invasive" surgical techniques. Over this time, multiple minimally invasive techniques have been described. Of these many procedures, two techniques have become popular and well studied - Minimally Invasive Video Assisted Thyroidectomy (MIVAT) and Transaxillary Endoscopic Thyroidectomy, with or without robotic assistance. Both are available here at the Medical University of South Carolina.
MIVAT was developed for thyroid nodules but soon the technique was expanded for use in early thyroid cancer and even central compartment dissections. Multiple groups have reported on the safety and efficacy of the procedure. In this technique, a 15 to 25 mm horizontal cervical incision is used. The thyroid gland is then mobilized using an endoscope, and the dissection is carried out as it is for a classical thyroidectomy (Figure 1). The main advantages are smaller incisions, less pain and shorter hospital stays.
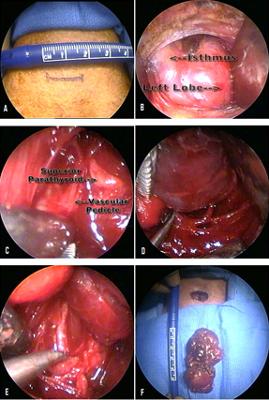
Figure 1. A. Incision; B. Exposure via the midline raphe; C. Superior pedicle dissection; D. Inferior pedicle dissection; E. Recurrent laryngeal nerve dissection; F. Removed specimen.
Transaxillary Endoscopic Thyroidectomy, with or without robotic assistance is the latest progression in the evolution of thyroid surgery, and has taken the "minimally invasive" concept to its extreme by providing for "scarless" thyroid surgery. The best studied example of this is transaxillary endoscopic/robotic thyroidectomy. In this procedure the surgical access is thru the axilla, and the surgery can be done with standard endoscopic instruments or the da Vinci Surgical System. It has become popular in the past decade in Korea and Japan because it completely avoids a neck incision. When compared to open thyroidectomy, preliminary experiences have shown a comparable rate of complications and surgical completeness with superior cosmesis. Joshua D. Hornig, MD, FRCS(C) performs the tranxaxillary approaches at MUSC.
 Figure 2. Transaxillary robotic thyroidectomy
Figure 2. Transaxillary robotic thyroidectomy
A. Approach B. Robot in use
Both of these procedures allow patients with thyroid nodules or early thyroid cancer to be treated in a minimally invasive manner. Therefore, patients benefit from decreased cost, decreased pain and better cosmesis. Best of all, over half the patients who require thyroid surgery are eligible for the procedure, and MUSC is the only hospital offering these revolutionary techniques in the region. For more information, contact us at headneck@musc.edu or call 843-792-8363.


