|
|

International Newsletter and Forum on Rigid Gas Permeable Contact Lenses, Corneal Shape, Health and Vision |
|
|
|
|
|
|
|
|
|
|
Vision by Design
 Vision by Design is the intriguing name of the conference by the orthokeratology academy of America, which celebrated its tenth anniversary in Phoenix (USA) recently. 'Vision by Design' refers to reshaping the cornea purposefully with orthokeratology, and hence changing the prescription by lens design. But a new dimension can be added to that: the ability to reduce the progression of myopia with orthokeratology lenses in children who have developing myopia. We don't have all the answers yet when it comes to the optimal peripheral amount of plus correction and the location of the specific correction (e.g. the optimal optical zone size, for instance). But current knowledge shared from the podium at the outstanding Vision by Design meeting was that we need a fair amount of 'near add' in the periphery to support a myopia reduction effect. Often we get children in our practices with a small amount of myopia. Orthokeratology can easily correct this, but typically does not create enough 'near add' in the periphery for optimal myopia progression reduction. From the podium, it was advised in lower degrees of myopia to start off with a high-plus periphery, center-distance soft lens. In the range of 2.5D to 6D of myopia, orthokeratology may prove to be the best option currently available for myopia progression reduction in children. Beyond -6D, orthokeratology has major limitations, and again alternative methods such as the mentioned center-distance soft lens should be considered. This certainly comes down to 'Vision by Design,' and it may reshape our profession. Eef van der Worp
|
|
(R)GPs for the dry patient?
 Ashley Wallace-Tucker and Kelly Nichols in Contact Lenses Today opened up the discussion as to whether (R)GPs are a viable option for our dry eye patients. It is commonly known that approximately 50% of all contact lens wearers suffer from dry eye. The vast majority of recent research has been focused on soft contact lens-related dry eye because this lens type dominates the market. However, some believe that R(GP) lens wearers have fewer symptoms of dry eye, the authors state. Oxygen transmission (Dk/t) and tear exchange are better with (R)GPs than with soft lenses, which may contribute to a successful use of these lenses in dry eye patients. Although specific studies are needed on the topic - the dry eye experts suggest not to exclude (R)GPs for this purpose and to consider them as a viable option. |
|
Stem Cell Deficiency and Keratoprosthesis
Loretta B. Szczotka-Flynn in her column in Contact Lenses Today raised an interesting point regarding using scleral lenses for limbal stem cell deficiency. Published case reports by Schornack et al and Rathi et al in international refereed journals show that scleral lenses may not only relieve pain and offer temporary protection, but they also may help improve the long-term condition in a constructive way. Scleral lenses provide protection to the epithelium from the lids' shear forces and provide continuous corneal hydration while being worn.
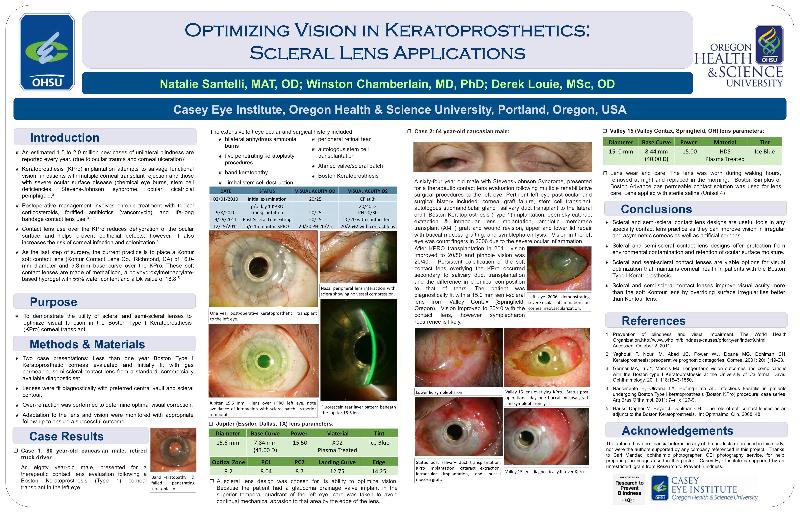
Another interesting topic regarding the use of scleral lenses is their use after keratoprosthesis. Keratoprosthesis implantation attempts to salvage functional vision in patients with multiple corneal transplant rejections and those with severe ocular surface disease such as chemical eye burns, stem cell deficiencies, Stevens-Johnson syndrome and ocular cicatricial pemphigoid. Standard of care is to use a large diameter soft contact lens over the keratoprosthesis to reduce dehydration of the ocular surface and to help prevent epithelial defects; however, this also increases the risk of corneal infection. A poster by Natalie Santelli, which won the clinical poster prize at the recent Global Specialty Lens Symposium, looked at the use of scleral lenses for that purpose. Scleral and semi-scleral contact lenses improve visual acuity more than soft lenses do by better overriding surface irregularities compared to soft lenses, according to the poster. They may be a good alternative to soft lenses in some cases. See link below for the full poster in PDF format.
Natalie Santelli, GSLS 2012 poster
|
|
Detour

Some patients may have one or more scleral conditions that interfere with a scleral lens fit. Most commonly these obstacles include pinqueculas and conjunctival blebs secondary to trabeculectomy. Our patient had a successful penetrating keratoplasty, but residual irregular corneal astigmatism had left her with 20/300 best corrected visual acuity. She also had a moderate conjunctival bleb located near the limbus at the 12 o'clock position from a previous trabeculectomy surgery to manage glaucoma. It can be difficult to successfully fit patients who have corneal irregularity and a conjunctival bleb with corneal (R)GP lenses. This is especially true if the bleb is located at the limbus because it can cause the lens to displace or dislodge. Additionally, the bleb is at some risk for damage if the corneal (R)GP lens edge repeatedly bumps into it with on-eye movement. An alternative approach for these patients is to fit them with a notched scleral lens. After 4 months of lens wear, our patient was successfully using the lens without any secondary corneal or bleb complications. Click here for the full report.
|
|
Smiley Face

A post-radial keratotomy patient reported poor visual acuity with his glasses. His prescription was OD +5.00=C-4.00x80 VA 0.5 and OS +5.00+C-6.00x80 VA 0.6. But from the moment the first trial lens as shown in the picture was applied, the vision with a mini-scleral lens (VA 0.8 and 1.0) made the patient smile. Photo: Jose Javier Rodriguez from the optometry school in Seville (Spain).
|
|
Upcoming Events
- Orthokeratology Society of Oceania, July 6-8, Gold Coast AU
- ISCLS congress 2012, September 7-12, Kent UK
- ECLSO congress, September 14-16, Nice FR
- ISCLS congress 2012, September 7-12, Kent UK
- VDCO Contact 2012, October 5-7, Friedrichshafen DE
- AAO, Oct 24-27, Phoenix US
- CCLS Symposium December 1-2, Houston US
|
|
|
|
|
|
|
I-site is an educational newsletter that is distributed on a monthly basis and provides an update on rigid gas permeable related topics (scientific research, case reports and other publications worldwide). I-site is objective and non-political. Its editor Eef van der Worp, optometrist, PhD, FAAO, FBCLA, FIACLE, FSLS is a lecturer for a variety of industry partners, but is not related to any specific company. Please contact us at: i-site@netherlens.com.
|
|
|