|
|

International Newsletter and Forum on Rigid Gas Permeable Contact Lenses, Corneal Shape, Health and Vision |
|
|
|
|
|
|
|
|
|
|
Momentum

What do orthokeratology, scleral lenses and Obama have in common? They all have gained, or are gaining, a lot of momentum. During the last presidential campaign in the USA, the word 'momentum' really became quite fashionable. Orthokeratology gained a lot of momentum exactly 10 years ago, although the word 'momentum' was not quite that popular then. Orthokeratology got attention in the media - for sure in my home country the Netherlands - which included national television coverage. But also worldwide there was a lot of 'momentum' with Global (and national) orthokeratology symposia, etc. Unfortunately, there was some sort of a setback on an international level, especially in parts of Asia, mostly because of suboptimal fitting and care standards but also because of a lack of understanding and knowledge about the concept. With today's research we now know what we perhaps should have known back then. Whether we like it or not, I do see some parallels with scleral lenses today. It is fascinating to see that scleral lenses get the attention that they do, as I think that there are many patients around the world who could seriously benefit from scleral lenses (also see the next item). But we should be careful not to get ahead of ourselves. There are a lot of questions to be answered on corneal (and scleral/conjunctival-) health and also on anterior ocular shape. In classical mechanics, momentum can be defined as Newton's second law. Let's see if we can get some more science behind scleral lens fitting, too.
Eef van der Worp
|
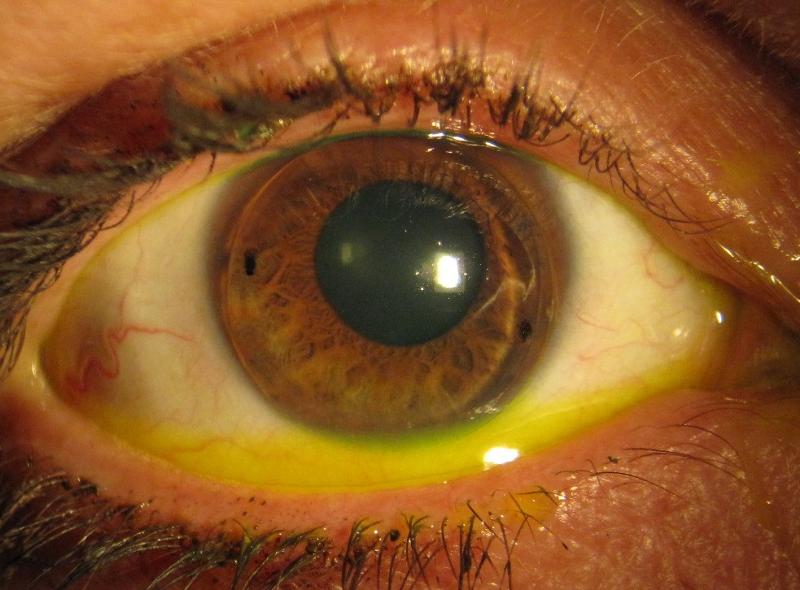
 The New Zealand National Eye Bank was analyzed for a 10-year period from 1994-2003 to identify potential donor, recipient, surgical and postoperative factors that may influence survival and visual outcome of penetrating keratoplasty (PKP). During this period, 1,820 corneas were supplied by the eyebank for PKP, and 1,629 (90%) had 1-year follow-up data. Overall, the 1-year survival rate was 87% (n = 1429). Keratoconus and Fuchs' endothelial dystrophy were the diagnoses with best survival and visual outcomes, whereas bullous keratopathy, trauma and noninfective keratitis were associated with poorer visual outcomes. For more risk factors, including graft size and neovascularization, see the article by Patel et al in the January 2011 issue of Cornea. A study by Borderie et al found the survival rate of penetrating corneal grafts to be 74 percent after five years, 64 percent after 10 years, 27 percent after 20 years and 2 percent after 30 years Ophthalmology, December 2009. For some patients lamellar procedures may therefore be the preferred technique of choice, although suboptimal visual outcome continues to be a concern. In any case, it seems advised for practitioners to explore all contact lens options prior to referring for surgery; whether they fit the lenses themselves or refer patients to a specialized colleague. The New Zealand National Eye Bank was analyzed for a 10-year period from 1994-2003 to identify potential donor, recipient, surgical and postoperative factors that may influence survival and visual outcome of penetrating keratoplasty (PKP). During this period, 1,820 corneas were supplied by the eyebank for PKP, and 1,629 (90%) had 1-year follow-up data. Overall, the 1-year survival rate was 87% (n = 1429). Keratoconus and Fuchs' endothelial dystrophy were the diagnoses with best survival and visual outcomes, whereas bullous keratopathy, trauma and noninfective keratitis were associated with poorer visual outcomes. For more risk factors, including graft size and neovascularization, see the article by Patel et al in the January 2011 issue of Cornea. A study by Borderie et al found the survival rate of penetrating corneal grafts to be 74 percent after five years, 64 percent after 10 years, 27 percent after 20 years and 2 percent after 30 years Ophthalmology, December 2009. For some patients lamellar procedures may therefore be the preferred technique of choice, although suboptimal visual outcome continues to be a concern. In any case, it seems advised for practitioners to explore all contact lens options prior to referring for surgery; whether they fit the lenses themselves or refer patients to a specialized colleague.
|
|
Hyper about Orthokeratology?
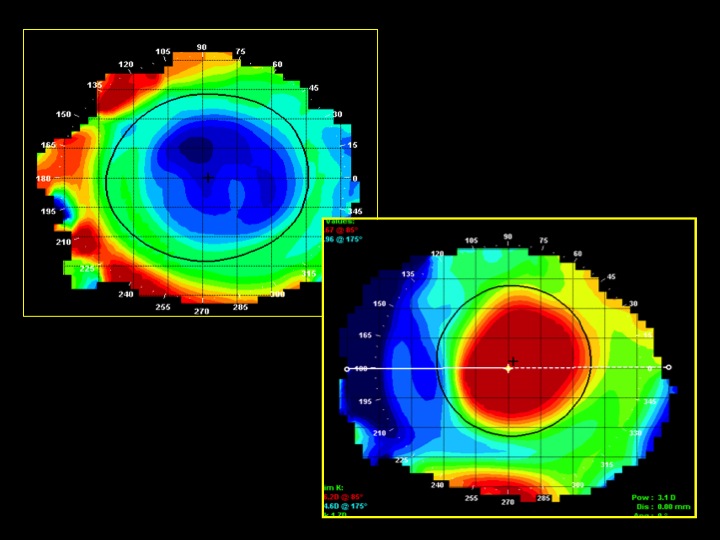
Hyperopic corneal reshaping was in the news. Luigina Sorbora and Genghe Lu published an article in Eye & Contact Lens showing that the hyperopic lens design they used, indended to correct +3.5D of hyperopia, induced a mean increase of 1.50 ± 1.87D change in refractive power after one night of wear. Paul Gifford presented his PhD thesis on this topic at the Global Specialty Lens Symposium (GSLS); he concluded that hyperopic corneal reshaping can be done successfully, but only to a certain level just as in myopic corneal reshaping. Up to +1.5D of correction seems fairly well controlled and predictable, but this appears to be less the case at +3.5D, he found. A new study of Gifford published in the March issue of Investigative Ophthalmology & Vision Science showed that para-central thinning of the cornea explains the topographical steepening in hyperopic orthokeratology and the refractive change. Whereas corneal thickening appears to be an additional factor in myopic orthokeratology, this was not the case in hyperopic treatment. This may at least partly explain the limitations of the amount of hyperopic orthokeratology that can be reached.
|
Myopia Control & Contact Lenses
| |
|
Myopia Epidemic
 A study by Zhang et al in China published in the October 2010 issue of Investigative Ophthalmology & Vision Science in 2010 found that 48.5% of Chinese children (mean age 13.7 years) had a spherical equivalent refraction of -2D or more. At the GSLS, the question 'The Myopia Epidemic - can it be managed or controlled?' was addressed. A 7-year study in Clinical Optometry (full access) on myopic orthokeratology showed a -0.37 ± 0.49D myopic change in a corneal reshaping group versus -2.06 ± 0.81D in a single-vision spectacle lens wearing group, but no eye elongation data was reported in this study. Relative peripheral hypermetropia seems to be at least one factor in driving myopia development that we may be able to influence. Jaume Pauné et al from Spain won third prize for their poster on the 'Performance of a New Special GP lens Design for Myopia Control to Produce Peripheral Myopization' at the GSLS meeting. They found in their experiment special (R)GP lens designs to effectively influence peripheral refraction and potentially reduce myopia progression. A recent study by Mutti et al from the Ohio State University (USA) in the January 2011 issue of Investigative Ophthalmology & Vision Science did find relative peripheral hypermetropia to have only a little effect on myopia development in a group of 2,043 children with a mean age of 8.8 ± 0.52D at baseline. Obviously, we don't have all the answers yet. Much more on this topic will be discussed at the upcoming Orthokeratology Academy of America meeting 'Vision by Design'. A study by Zhang et al in China published in the October 2010 issue of Investigative Ophthalmology & Vision Science in 2010 found that 48.5% of Chinese children (mean age 13.7 years) had a spherical equivalent refraction of -2D or more. At the GSLS, the question 'The Myopia Epidemic - can it be managed or controlled?' was addressed. A 7-year study in Clinical Optometry (full access) on myopic orthokeratology showed a -0.37 ± 0.49D myopic change in a corneal reshaping group versus -2.06 ± 0.81D in a single-vision spectacle lens wearing group, but no eye elongation data was reported in this study. Relative peripheral hypermetropia seems to be at least one factor in driving myopia development that we may be able to influence. Jaume Pauné et al from Spain won third prize for their poster on the 'Performance of a New Special GP lens Design for Myopia Control to Produce Peripheral Myopization' at the GSLS meeting. They found in their experiment special (R)GP lens designs to effectively influence peripheral refraction and potentially reduce myopia progression. A recent study by Mutti et al from the Ohio State University (USA) in the January 2011 issue of Investigative Ophthalmology & Vision Science did find relative peripheral hypermetropia to have only a little effect on myopia development in a group of 2,043 children with a mean age of 8.8 ± 0.52D at baseline. Obviously, we don't have all the answers yet. Much more on this topic will be discussed at the upcoming Orthokeratology Academy of America meeting 'Vision by Design'.
|
|
A lengthy study

With all the turmoil regarding myopia control and axial length in normal ametropic patients, it was interesting to see a study on axial length in keratoconic eyes. Ernst and Hsu reported a study in Eye & Contact Lens showing that the axial length, the anterior chamber depth, and the posterior segment length were all significantly longer in keratoconic patients than in emmetropic patients. The mean keratometric values for the keratoconic group did not correlate with axial length. This finding that keratoconic eyes seem to have longer axial lengths on average, primarily because of longer posterior segment lengths than emmetropic eyes, can be of value for patients undergoing keratoplasty because it relates to post-keratoplasty refractive outcomes, the authors concluded. Another study by Atchinson et al in Investigative Ophthalmology & Visual Science looked at peripheral ocular aberrations in mild and moderate keratoconus. Most research to date in keratoconus has been focused on axial aberrations. This study also found significant differences in peripheral aberrations in the moderate versus mild keratoconic eye as well as in the keratoconus group versus the emmetropic group.
|
|
An Extra Step
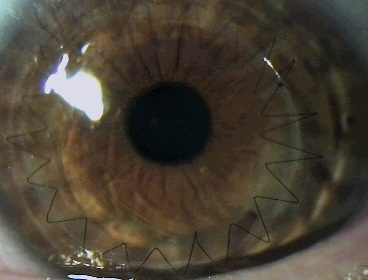
A patient presented with mild keratoconus in her right eye and was diagnostically fit with a bi-aspheric large diameter (R)GP lens. Although the lens fit well, it only provided the patient with 20/50 vision. The result of a sphero-cylindrical over-refraction was +2.00 -1.25 X 105. A front surface toric lens was ordered and dispensed with a power of -2.00 -1.25 X 105 that was stabilized with double slab-off, which gave the patient 20/25 vision. Keep in mind that it may be necessary to take an extra step to maximize a patient's vision when using (R)GP lenses to correct for corneal irregularity.
I(n)-site-the-practice by Greg DeNaeyer
|
|
The Art of Vision
Many specialty lens practitioners are less and less wavery about incorporating wavefront technology into their practices. Diagnostically a very powerful instrument, it also has more and more applications in terms of explaining and implementing vision correction options
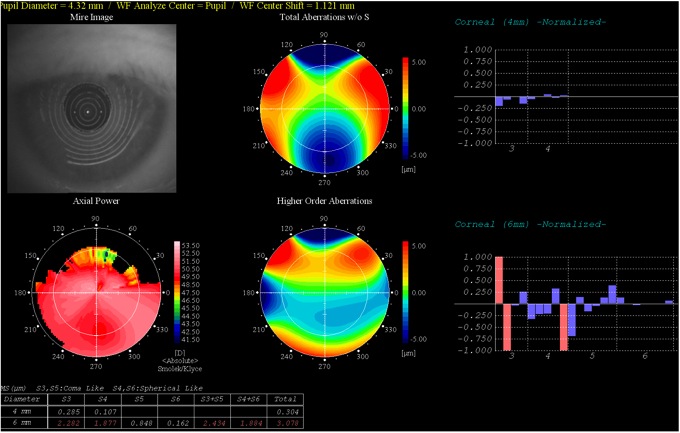 | |
Picture: Carolien Kunnen
|
The picture above represents an overview of a keratoconic eye: it shows the Placido image of the cornea at the top left, axial corneal topography power map on the bottom left, total aberrations of the eye in the top middle and the higher order aberrations in the lower middle image. On the right, the corneal aberrations (in graph) are shown with a 4mm and a 6mm diameter area (Topcon Wave-Front Analyzer). Many corneal higher order aberrations can be corrected with (R)GP lenses if the lens centers well.
|
|
Upcoming Meetings
- Vision Expo East, March 16-20, New York USA
- Cornea & Contact Lens conf, March 31-April 3, Queenstown NZ
- Vision By Design, April 29th - May 1st, Orlando USA
- EFCLIN, May 12-14, Barcelona ES
- BCLA conference, May 26-29, Manchester UK
- AOA meeting, June 15-19, Salt Lake City USA
|
|
|
|
|
|
|
I-site is an educational newsletter that is distributed on a monthly basis and provides an update on rigid gas permeable related topics (scientific research, case reports and other publications worldwide). I-site is objective and non-political. Its editor Eef van der Worp, optometrist, PhD, FAAO, FBCLA, FIACLE is a lecturer for a variety of industry partners, but is not related to any specific company. Please contact us at: i-site@netherlens.com. |
|
|

